Forty Years Late: Why So Many AuDHD, ADHD, and Autistic Adults Are Only Now Getting the Right Diagnosis
A client comes to me at forty-one with a diagnostic history longer than her résumé. Her story is not rare — it is close to the median story for adults who are only now getting an accurate neurodevelopmental diagnosis.

Forty Years Late: Why So Many AuDHD, ADHD, and Autistic Adults Are Only Now Getting the Right Diagnosis
A client comes to me at forty-one with a diagnostic history longer than her résumé. Generalized anxiety at nineteen. A brief, uncertain flirtation with a bipolar II label at twenty-four, dropped when the mood stabilizer did nothing. Borderline personality disorder at thirty, a label she carried for a decade like a verdict. She has been, by her own account, in some form of treatment for over twenty years, and not one clinician in that span ever asked her about sensory overwhelm, or special interests, or what happens in her body during unstructured social time. She was diagnosed with both ADHD and autism last year. She describes the assessment as the first time a clinician had ever actually seen her.
This is not a rare story. It is close to the median story for adults — disproportionately women, disproportionately genderqueer and nonbinary people, disproportionately LGBTQIA2S+ folx more broadly, disproportionately people of color, disproportionately anyone who learned early that performing normalcy convincingly was the price of being taken seriously — who are only now, in their thirties, forties, and fifties, getting an accurate neurodevelopmental diagnosis. Understanding why it took this long is not just an interesting side note. It's clinically necessary, because a client's twenty-year misdiagnosis history isn't background information. It's part of the injury.
The DSM Made This Structurally Inevitable
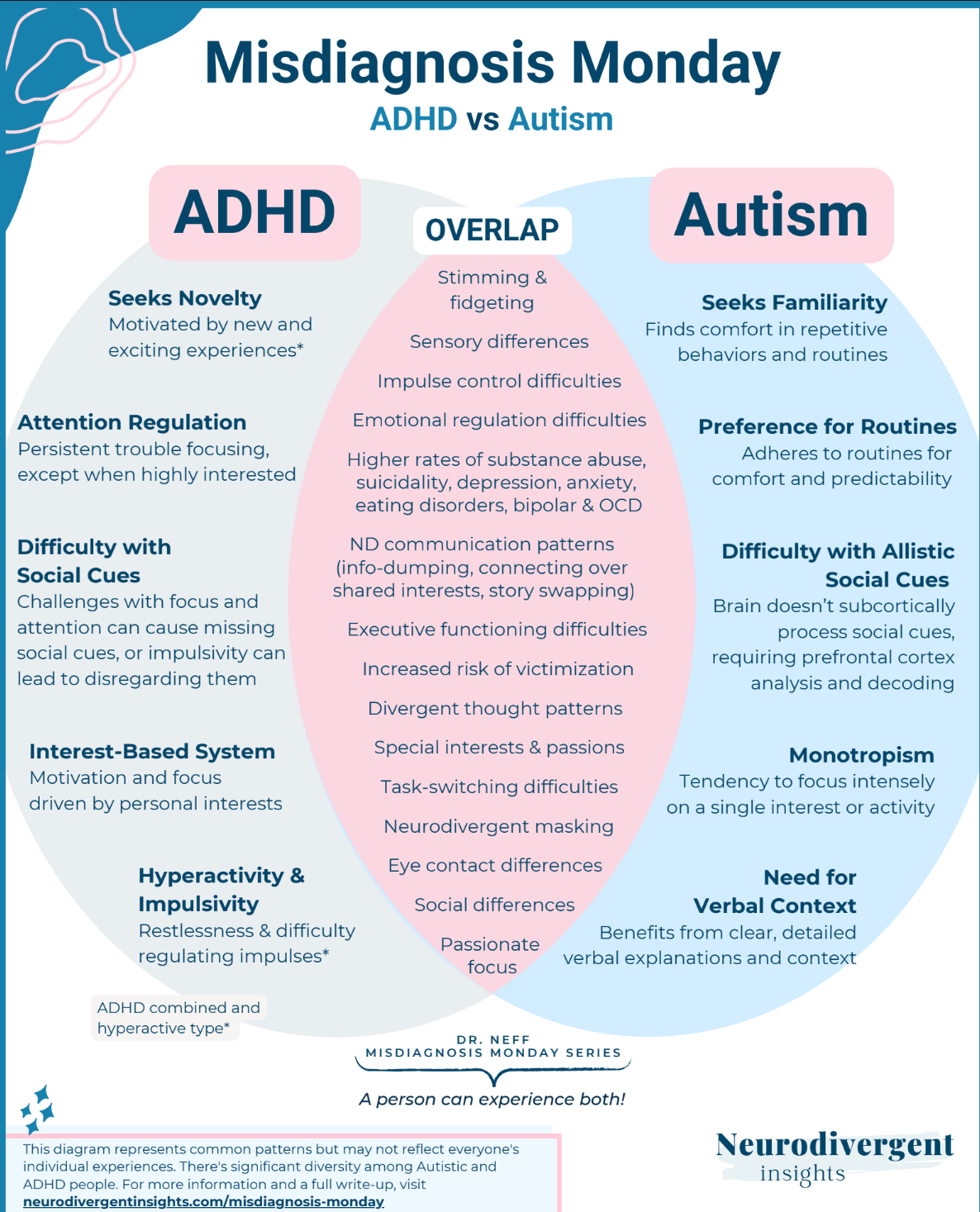
Here's a fact that surprises most clients, and more than a few clinicians: until the DSM-5 was published in 2013, it was formally, diagnostically prohibited to give someone both an ADHD diagnosis and an autism diagnosis. The DSM-IV exclusion clause explicitly listed pervasive developmental disorders as an exclusion criterion for ADHD — if a clinician suspected autism, they were barred from also diagnosing ADHD, regardless of what was actually in front of them.
This wasn't a minor technicality. Research at the time already suggested that a substantial portion of autistic children had clinically significant attention and hyperactivity symptoms, but the manual made it diagnostically impossible to name both. Clinicians describe having to write around it — calling documented ADHD symptoms "ADHD-like features of autism" in charts and research, because the actual label wasn't available to them.
The exclusion was lifted in 2013, less than fifteen years ago. Anyone diagnosed, assessed, or simply overlooked before that point was evaluated inside a system that could not, by design, see the whole picture. And because so much of adult diagnosis depends on developmental history — what did this look like when you were seven — a huge number of adults now in their thirties, forties, and fifties had their entire childhoods assessed, if they were assessed at all, under a framework that had already decided their two sets of traits couldn't coexist. AuDHD, as a coherent, nameable profile, simply did not officially exist for most of these clients' developmental years.
Bias in Who Gets Seen, and Why Intersection Compounds It
The diagnostic criteria most clinicians were trained on were built from research populations that were overwhelmingly young, white, and male. Leo Kanner's and Hans Asperger's original case studies, and decades of research that followed, centered boys almost exclusively, and the resulting criteria reflect what autism and ADHD look like in that specific, narrow population far more reliably than they reflect anyone else's presentation.
Women and girls are diagnosed later, less often, and frequently only after a cascade of other labels first. Genderqueer and nonbinary people face the added layer of clinicians who may already be struggling to separate gender identity from presentation. LGBTQIA2S+ folx more broadly often learn camouflaging for a related but distinct reason: a childhood and adolescence spent monitoring every gesture, interest, and inflection for anything that might read as different in a hostile environment builds exactly the kind of hypervigilant social masking that can bury a neurodevelopmental profile underneath what looks, from the outside, like a personality shaped entirely by being closeted.
Clinicians frequently attribute the anxiety, the hyperawareness, the exhaustion after socializing, entirely to minority stress, without ever asking whether a second, co-occurring explanation is sitting underneath it. People of color face documented diagnostic disparities on top of all of this — Black and Latino children, for instance, are consistently identified and diagnosed later than white children with clinically comparable presentations, often only after behavior has been mislabeled as a discipline problem rather than a clinical one.
None of these are separate, parallel problems. They compound. A queer woman of color is not simply facing three independent chances of being missed — she's facing a diagnostic system where each additional distance from "young white boy" stacks the likelihood of being overlooked higher than any single factor would predict on its own.
Camouflaging and the Masking Problem
Camouflaging — the effortful, often unconscious masking of autistic or ADHD traits to blend into a given social environment — is more heavily socialized into anyone whose survival has depended on reading a room correctly, which reliably includes women, LGBTQIA2S+ and gender-nonconforming people, and people of color navigating majority-white or majority-cisheteronormative spaces.
It's extremely effective at hiding the underlying profile from clinicians trained to look for a much narrower, more stereotypical presentation. The traits didn't hide. The diagnostic framework simply wasn't built to see them, and it was built least of all to see them in anyone holding more than one marginalized identity at once.
The Comfort of Familiar Labels
Ask most clinicians whether they're comfortable diagnosing a mood disorder, bipolar disorder, or borderline personality disorder, and the answer is generally yes, without much hesitation. Ask the same clinicians about diagnosing adult autism or ADHD, and a striking number will describe hesitation, self-doubt, or an instinct to refer out.
Some of this is genuinely about the added burden of standardized testing that formal autism assessment often involves. But a meaningful part of it is subconscious bias operating exactly the way it does everywhere else in clinical work: pattern-matching to the label that's most cognitively available, most trained-on, most familiar, rather than the one that's most accurate.
When the picture is ambiguous, clinicians tend to default to whichever diagnosis they trained on most, and that default has a documented cost: years, sometimes decades, of a client being treated for the wrong thing.
What the Delay Actually Costs
None of this is abstract for the client living through it. Every year spent inside the wrong diagnostic frame is a year spent in treatment that doesn't fit — DBT skills built for emotional dysregulation that was never the actual mechanism, medication trials for a mood disorder that was never quite right, and beneath all of it, the compounding exhaustion of the boom-or-bust cycle: pushing through on the good days because that's what the treatment plan implicitly demands, crashing afterward, and never being handed a framework that actually matches how their particular nervous system spends and recovers energy.
A client managing undiagnosed AuDHD isn't failing to respond to treatment. They're often being asked to pace a body running on rules that were never written for it.
The forty-one-year-old client I described at the start didn't need twenty more years of a diagnosis that almost fit. She needed one clinician willing to ask a different set of questions, and confident enough in their own license to act on what the answers actually showed. That's a lower bar than the field has been treating it as, and closing that gap is, at this point, mostly a matter of will.
Well wishes.
Mx. Love C. Dialogos, LMFT — Licensed Marriage and Family Therapist | Buddhist Chaplain
The client described at the opening of this piece is an illustrative composite, not an account of any specific individual. This article is for educational purposes only and is not a diagnostic tool. If you recognize your own history in this piece, please bring it to a licensed clinician for a real evaluation rather than self-diagnosing from an article.
Further reading on this site:
- Neurodivergence and Suicide: Why Autism and ADHD Predict Risk Through Different Mechanisms — the two distinct pathways, and why late diagnosis raises risk
- Autistic Burnout: Definition, Causes & Suicide Risk — what happens when masking goes on too long
- Rejection Sensitive Dysphoria: What It Is and Isn't — the ADHD emotional dysregulation piece that often gets missed
- The Neurodiversity Paradigm: A Sociological History — where the framework underlying all of this actually came from
Explore Topics
Written by
Mx. Love C. Dialogos, LMFT
Content creator and writer sharing insights and stories.
© 2026 Love Psychotherapy, LLC. All rights reserved. Love Psychotherapy® is a registered trademark.


